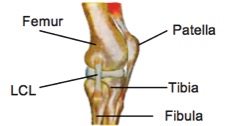
The knee is one of the largest joints in the body and has only one plane of movement. This means it bends and straightens but does not twist (much) or move from side to side. To keep the knee from moving in other directions, the knee is supported by many strong ligaments, with two of these being found on either side of the knee. The inside ligament is the ‘Medial Collateral Ligament’ (MCL) and the outside one is the ‘Lateral Collateral Ligament’ (LCL). The primary role of the LCL is to prevent the lower leg from moving too far towards the midline in relation to the upper leg. Both the LCL and MCL are extremely strong ligaments and provide lots of support to the knee during movement however, they are still vulnerable to injury.
How do tears happen?
The LCL is injured less often than the MCL, however tears do still occur. The most common way the ligament is damaged is through a force causing the knee to move inwards in relation to the upper leg, or a twisting of the knee. This can be seen in sports that involve changing directions or with a direct force, such as a rugby tackle. This injury can also occur from a simple fall and as with all sporting injuries, it is not only athletes who can be affected, anyone can tear their LCL in the right circumstances.
What are the symptoms?
Following an injury to the LCL, common signs and symptoms are a ‘popping’ sound at the time of injury, immediate pain with weight bearing and swelling and a feeling instability. The severity of the injury will impact how much each of these symptoms are felt and LCL tears are classified as either Grade I, II or III, which helps to direct treatment. A grade I tear is where a few fibers of the ligament are stretched and damaged, a grade II is where this a partial rupture of the ligament with some instability of the knee and Grade III is a complete tear.
How are LCL tears diagnosed?
Your physiotherapist is able to perform clinical tests to evaluate if there is any instability of the knee from an LCL tear. An MRI can confirm this diagnosis and an X-ray may be required to rule out any associated fracture. It is possible for nerve damage to occur at the same time as an LCL Tear, which will result in weakness and loss of sensation in the lower leg. Severe injuries are more likely to involve injury to other parts of the knee and your physiotherapist will make a full evaluation of all your injuries on assessment.
Most LCL tears are managed well with just physiotherapy and support of the joint, however severe tears and associated nerve damage may require surgery. Your physiotherapist and medical team will work together to help determine the best course of action for each individual injury.
How can physiotherapy help?
For tears that don’t require surgery, your therapist will advise you on how to best support and protect the injured joint. In the first 48 hours, RICE protocol (Rest, ice, compression, and elevation) is applied to reduce any pain, swelling, and inflammation. Following this period, you will be advised on how best to mobilise the joint whilst preventing any further damage. Return to sport will be dictated by healing times with a full recovery expected by 6-12 weeks.
Following ligament damage, balance, strength, and proprioception are often impacted and your physiotherapist will develop a program to address this, which is an important part of preventing further injury. Tears that are repaired surgically will require a longer program of rehabilitation and close liaison with the medical team.
None of the information in this blog is a replacement for proper medical advice. Always see a medical professional for advice on your individual injury.